I've always found going to the doctors a strange experience. Usually, it's a sore throat, sometimes something worse. I sit down, start explaining my problem to my doctor. They listen patiently and start taking notes, with this piece of software.
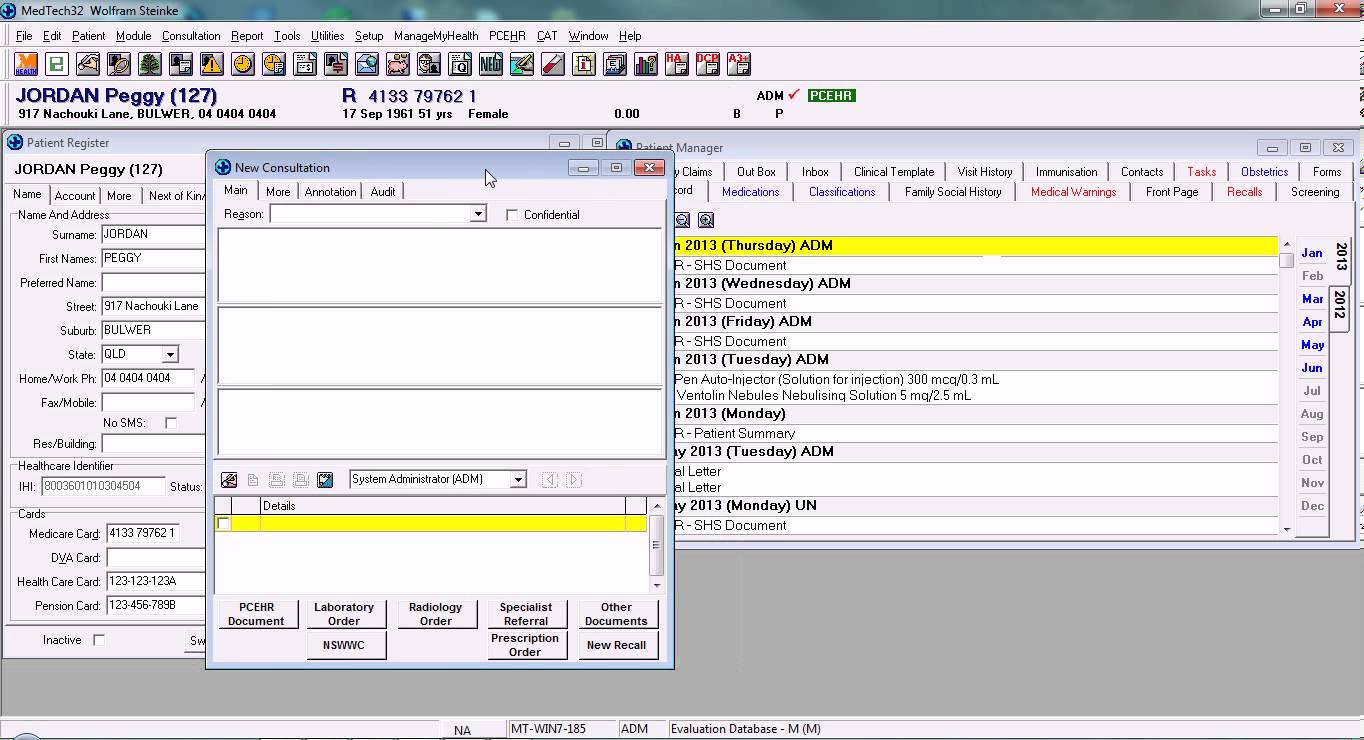
MedTech 32, Practice Management Software
This part always bothered me - because the software they use doesn't seem that great.
I'm a software developer and interface designer, so I am more sensitive than most. However, from my perspective as a patient, it never filled me with confidence. The software looks like it hasn't been upgraded since Windows XP. It doesn't look that easy to use. It makes me question how safe my data is. And most importantly, my medical record doesn't feel like mine. It's owned by that piece of software.
The bizarre part is, the doctor is fantastic. They have trained for over half a decade, have a wealth of knowledge and experience, and are supported by the most amazing technology. Decades of drug research and advancement, only a prescription away. Almost any biological sample you can produce, blood, urine, swabs, can be tested for disease. X-Rays, MRI scans, Ultrasound - they can gain a perspective of you nobody else can. They are such a contrast to the tool they use every single day, for every single appointment - which appears to have completely missed this technological advancement.
It turns out I'm not the only person to think this - every doctor I have talked to has been dissatisfied with the state of healthcare software. Some doctors are even writing songs about how bad their software is.
"They built you a turd, doc" - ZDoggMD
At this point you have to think, why is this? Why is healthcare software so bad? Considering medical professionals training, and responsibility, it makes sense that they'd have nothing but the absolute best software we can build?
The Challenge
It would be foolish to think nobody has tried to solve this issue before. The truth is, many people have tried to improve healthcare software, and many have failed.
In 2002 the UK Government decided they needed to build an Electronic Health Record (EHR) system for their citizens. They dreamed of connecting all of their healthcare institutions together, from primary care (community doctor's clinics) to hospitals, to pharmacies. This system was going to store patient records, manage electronic prescriptions, handle patient appointments and more. It was going to revolutionise the UK's healthcare system.
It was a complete failure. The project was originally going to cost £2.3 billion ($7.8 billion NZD), and take three years. However, nearly ten years later, and £12.4 billion ($27.2 billion NZD), their goals were not met (National Audit Office, 2006). They had failed to finish most of the project, and the parts they had weren't getting any real world use. The majority of their investment was written off, wasted, and the project was shutdown in 2011 (Department of Health, 2011). It was arguably, one of the largest IT failures in the world.
It can be hard to comprehend how much a billion is. But considering that a qualified nurse starts at around £21k per year ($36k NZD), over the ten years they could've spent that money on 44 thousand extra nurses.
Of course, perhaps its easy to see how a bureaucratic government process could chew through money. Maybe they needed to leave it up to a competitive market, and let the best software win? This was exactly what America did (Robert, 2015). They decided to provide a stimulus package of $30 billion USD - to pay software vendors to improve their software, and pay institutions to start using it.
Their goal was to computerise the healthcare system, and the usage of computers did increase dramatically. However, the quality of their software, Robert argues, is not worth $30 billion USD. They now have a system where there are many different products, all with different formats, and getting them to cooperate is a huge challenge. The previous director of America's health IT office (before the stimulus package), said:
"We've built the Frankenstein I was most afraid of" David Brailer
Private institutions in America have also faced huge costs when implementing large Health IT projects. Hospital chain Kaiser Permanente, spent 10 years and $4 billion dollars on their EHR system - about $444 per registered patient (Snyder, 2013).
A smaller chain Partners spent $1.2 Billion on their EHR - a cost of about 2 million dollars per doctor (McCluskey 2015). While both these institutions found success with their new software, the cost is still undeniably, immense.
The Question
The people who have tried and failed had a lot in their favour. They had experience in the healthcare industry. They had institutional support, from both medical institutions and government institutions. They had political power, and influence. And they had lots of funding, which they could use to get the absolute best people they could find.
But, with all that, they all had issues with cost, quality, or complete failure.
It makes you wonder - what were they missing? Why did they fail? Why did it cost so much? And the larger question - Why is good healthcare software so hard to create?
That is the topic of this thesis. I've spent the last 12 months trying to answer that question, while designing a radically different Electronic Health Record (EHR) system for primary care in New Zealand. But first, let me explain what an EHR system actually is.